All we have to do now is to answer the important question: The answer is YES and the consequences are SERIOUS.
The fact that these consequences are serious is easily explained: This leads unavoidably to loss of brain tissue. Where this loss occurs depends on the distribution of the blood vessels in the brain (the shape of the "arterial tree") which is almost certainly determined by hereditary factors.
The brain is the most important "computer" in our body; three functions can be localised in it:
The necrotic brain tissue is replaced by connective tissue, as a result of which the notorious plaques occur. This diseased tissue is also an ideal site for a virus to nestle. (Cf. the research by Dr H. van Noort of the Netherlands Organization for Applied Scientific Research (TNO), in Delft, an article in "Hersenwerk" ("Brainwork") 2 2002, Newsletter 28, of the Information and Education Worldng Group of the National Hersenwerk Committee 2002.)
If misalignments B and C are also combined with A, then the clinical picture is further complicated by depressive symptoms.
Owing to the very serious consequences, I have called homolateral A and B the Fatal Combination.
Contralateral misalignments A and B likewise have serious consequences, but these occur later and are much less drastic. I have called this the Serious Combination.
The question now is: In framing my answers to these questions I shall first discuss the Fatal Combination in relation to a number of clinical pictures.
The Fatal Combination with the depression position. Both schizophrenia and borderline syndrome can occur with the depression position. These patients are extremely suicidal. In my opinion, in this kind of disorders of a neurological and psychiatric nature these observations represent a serious incentive also to take a look under the skull instead of only inside it.
The time has now come to see whether results were achieved with the treatment. First, however, a few considerations which are applicable in this respect: apart from the depression position of C-1, which besides stimulating the ganglion cervicale superior also causes mechanical stimulation of the nervus vagus
(resulting in depression = vagotonia and anxiety and panic disorder = sympatheticotonia), the whiplash misalignments combined with the abnormal position of C-1 with the tongue bone phenomenon produce a sympatheticotonia and, consequently, vascular spasms - tissue degeneration - tissue necrosis. One patient confirmed my train of though in this regard: a young man entered my surgery as a zombie. On inquiry it turned out that he had schizophrenic symptoms (delusions, hearing voices, etc.) on account of which a psychiatrist had prescribed antipsychotics for him. He had visited my surgery because of neck complaints. He had none of the three abnormalities, only slight abnormal positions of C-2 to C-6. According to my understanding (cf. supra) he was not schizophrenic, so what was causing his condition? Incisive questioning produced the answer: he was addicted and was taking between half a gram and a gram of amphetamine daily! Amphetamine is a sympathomimetic which in overdose therefore produces the same symptoms as a mechanical stimulation of the ganglion cervicale superior! Very instructive. The longer this stimulation exists, the greater the tissue loss.
Are there indications that correction of the above-mentioned abnormal positions of the vertebrae result in the long run in improve in the aforesaid disorders?
The answer is: YES.
A discussion of the changes observed is given below. Unfortunately I cannot discuss all patients since a number have moved and I was unable to discover their new address, while others have been treated too recently to be able to expect results.
Furthermore, consideration should also be given to the fact that protracted abnormal positions can eventually produce substantial tissue degeneration. A recovery period can last years, especially in older patients.
Gilles de la Tourette syndrome: The young patients responded very positive after neck corrections.
Guillan-barre syndrome: male, 60 years old, degeneration of the muscles of the arms and legs, had to be assisted up stairs. Treated in November 1998. After six months the muscular atrophy was eliminated except for slight residual atrophy in the right hand. Now climbs the stairs two steps at a time. In Manic-depressives the manic phases cease (unless, of course, abnormal positions recur due to the patient bumping his head). The depression diminishes slowly, the attention focuses more on external events and new things are undertaken. Most patients can live without medicines and without emotional disorders.
The Schizophrenics I followed showed considerable improvement: delusions disappeared and the
voices ebbed away (certainly after the concomitant use of propranolol). Needless to say, a lot of effort is
required to resume a normal life. Nonetheless, my first patient has a job at a ministry and is no longer taking medication. Psychoses no longer occur, of course, unless the patient forcibly strikes his head again, as a result of which the ganglion cervicale superior is again stimulated by abnormal vertebral positions
With regard to Parkinson's disease, the course was as follows: a number of patients were operated, others had not worsened, and one patient really surprised me. This man (born in 1932) was treated in 1994 and in the spring of 1999 he no longer displayed rigidity or tremor. In this patient of the Leiden University Hospital the medication was stopped. He still displays a very slight dyskinesia.
The Borderline patients responded in the same way as the schizophrenic patients. The depression position tends to recidivism. An operative fixation of C-1/C-2 should be considered in such cases, since the ligamentum transervurn atlantis is probably excessively stretched. This operation was performed in rheumatic patients. Needless to say, the vertebrae must be fixed in the correct position!
Experience with Multiple Sclerosis patients is favourable: the process
stops. An improvement occurs, after which the situation remains static.
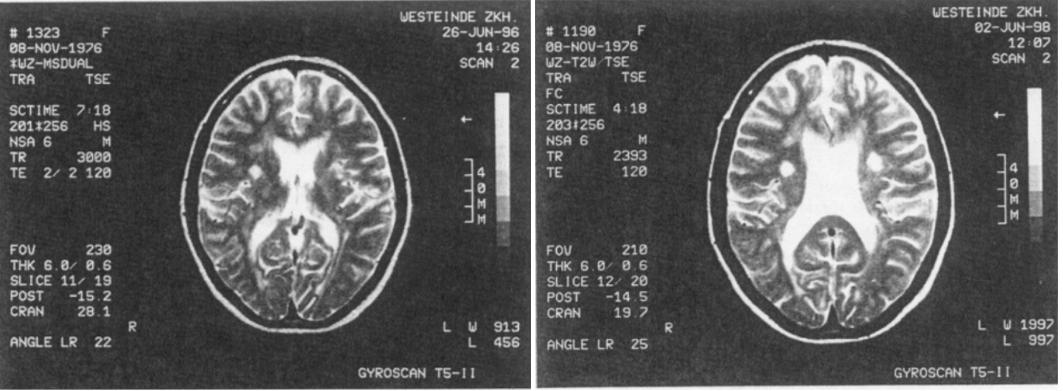
I was able to follow a female patient for many years. An MRI was made
of a 19-year-old girl one year prior to treatment who was suffering from
cerebral vomiting. This disappeared after a couple of months. The second
MRI, made six months after the treatment, showed a major improvement.
Today she is free of complaints. (see the photos).
The Alzheimer patients have been treated too recently for an assessment to be made.
The Phobia patients show a good improvement: the nightmares have disappeared and the anxieties have diminished. Their life has again acquired more "space".
The Bulimia patients responded immediately after the first treatment. The urge to eat decreased spectacularly and completely disappeared after several weeks.
Then, the Autistic patients. Here too, clear progress was made. Usually it takes several years, since a major retardation must be made good. A young girl with selective mutism has been cured.
Achievements at school and contacts with fellow students have generally improved. A 29-year-old autistic patient (who had in the meantime been declared schizophrenic without ever having been psychotic) now has a job with a municipal parks and playing fields department. About ALS: the observation time is too short for any conclusions for this moment.
We have now discussed:
Does a combination of these misalignments occur and, if so, what are the consequences?
When A and B are combined on the same side (which is usually the case) then C-1 is situated far in the ventral direction under C-0; this joint is fixed (no translation) while C-2 is positioned in the dorsal direction relative to C-3. This joint is also fixed (no translation). The processus transversi of C-1 and C-2 are therefore situated far apart from each other, the first in the ventral direction and the second in the dorsal direction, and joint C-1/C-2 is the only joint in this region where movement is possible. The ganglion cervicale superior, which is situated directly against these two transverse processes, is therefore subject to strong mechanical stimulation with every movement of the head. From this ganglion fibres go directly into the brainstem, but also to the arteria vertebralis and the internal carotid artery. The stimulation from this ganglion causes vascular spasms in the face (manifested by pallor) and in the brain and brainstem.
There is therefore a "link" with the incorporeal. With this combination one can therefore expect both neurological and psychiatric disorders depending upon the site where the tissue degeneration occurs.
In which disorders are these misalignments found, in how many persons and how large is the correlation between the clinical picture and the misalignments?
The Fatal Combination
Seven years ago I treated my first schizophrenic patient, a 21-year-old
male who had had some psychoses which started after a series of accidents.
I particularly noticed the serious misalignments high in the neck and
I suddenly had the idea that there might be a causal connection here.
Several other patients followed, especially after I had attended a meeting
of the Association of Schizophrenic Patients. At this meeting I was
allowed to examine everyone and I was told that one of them was not
schizophrenic. I was asked whether I could tell which of the fifteen
people present it was. I succeeded in doing this within fifteen minutes:
that person was the only one without the Fatal Combination. There
was a 100% correlation. A total of 87 patients were treated. All the
diagnoses were made by psychiatrists. 'Me onset of the illness usually
starts three to six months after the last accident.
All the diagnoses were made by neurologists. The correlation with the
Fatal Combination is 100%. Number of patients: 83. A striking aspect
is that the illness commences 15 to 20 years after the last accident.
All the diagnoses were made by neurologists. The correlation with the
Fatal Combination is 100%. Number of patients: 61.
All the diagnoses were made by psychiatrists. Number of patients: 14. Correlation: 100%. In addition to the Fatal Combination, they all had the depression position of C-1.
19 patients with the Fatal Combination diagnosis made by a psychiatrist.
Diagnosis made by a specialist or GP. Number of patients: 11.
The diagnosis was made by a specialist. Number of juvenile patients:
100. The seriousness of autism is congruent with the seriousness of the
high neck syndrome. Autists with the Fatal Combination as a rule
don't speak and start to speak after threatment. Autists with the
Serious Combination speak but live in their own world and are often
difficult to manage. Sometimes the autists have epileptic (Syndrom of
West). All change their manners in the currency of the year after threatment
Muscular atrophy with a high albumin content in the liquor. 4 patients. Diagnosis made by a neurologist.
All the diagnoses were made by psychiatrists, Number of patients: 22.
Correlation: 100%.
I only saw one patient with this condition.
13 patients. All had the Fatal Combination.
The Serious Combination
Moving on, I shall now discuss the Serious Combination (whiplash misalignment plus heterolateral tongue bone phenomenon).
This misalignment is apparently still serious enough to cause dementia
at an advanced age when it has existed long enough. Number of patients:
11. The patients had either the Fatal Combination or the Serious
Combination.
Number of patients: 36
9 patients, all with considerable overweight. One woman had the whiplash misalignment plus the depression position of C-1.
The other patients responded also positive after threatment.
Very striking was the change in a 6-year-old girl who was being treated in a Rotterdam hospital following diagnosis of West's syndrome. She had the tongue bone phenomenon with a depression position at the same side.One treatment was sufficient with a check-up after 14 days. Within a week her behaviour was totally changed and normalised. She was a vacuum-extraction victim.
Summary
The above findings are very serious indications that we are concerned here with a causal therapy which can prevent untold misery and expense. The forensic implications are also important. The diagnosis of schizophrenia is nolonger a question of conjecture but a queation of a scan followed by an MRI. Such an scan is shown here, a left-sided Fatal Combination. The displacement of the hyoid bone towards the left ahead of C-3 can be clearly seen.
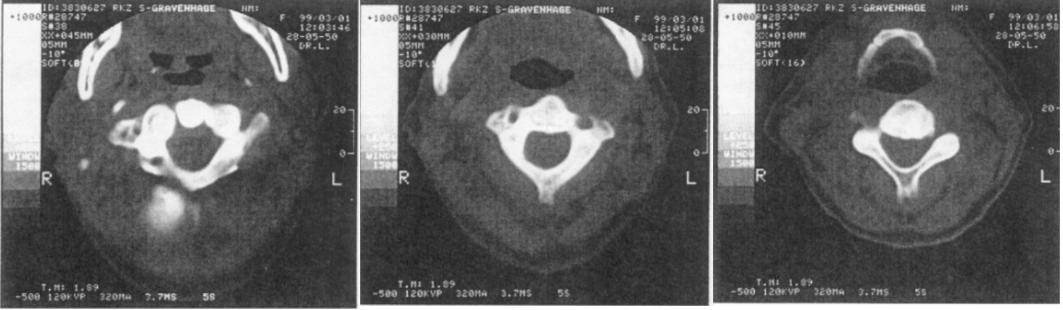
Again a serious warning: this image only appears when the patient's head is fixed in a straight position! If you fail to do this, the patient will immediatly turn his head to a position that he feels is 'straight'. As a result, the image is not seen and the diagnosis is missed.
Literature
- Mc Guire P.K. e.o. The neural correlations of inner speech and auditory verbal imagary in Schizofrenia. Relationship to auditory verbal hallucinations. Brit. journ. of Psych. 1996: 169, 149-159
- Chrishnan KRR e.o: MRI defined vascular depression. Am. journ. of Psych. 1997: 154, 497-50 1.
- Alexopoulos GS e.o. Clinical defined vascular depression. Am. journ. of Psych. 1997: 154, 562-565.
- Claus J.J. e.o.: Mesurement of temporal reginal cerebral perfusion with single photon emission tomography predicts rate of decline in language function and survival in early Altzheimer disease. Europ. journ. of Nucl. medicine. 1999: 26, 265-27 1.
| Autism | 91 |
| Parkinson's disease | 76 |
| M.S. | 53 |
| Manic-depressives | 21 |
| Asperger | 4 |
| Phobia | 29 |
| Alzheimer | 9 |
| A.L.S. | 12 |
| Gilles de la Tourette | 10 |
| Gaullian Barre | 3 |
| Schizophrenics | 79 |